Fevers
December 10, 2003
Past medical history is significant for obesity, end-stage renal disease due to hypertension, and glucose intolerance. He has a dialysis fistula in his right forearm which has been functioning. Last dialysis was yesterday.
He no longer smokes and denies alcohol intake. He is a retired bus driver and is married, with two children of his own and two stepchildren.
Family history is significant for a father who died from complications of diabetes.
On exam, he is in no distress.
Vital signs: BP 160/100, HR 120, R 16, T 102.8F.
Lungs are clear bilaterally.
Heart exam is normal.
Abdomen is soft. Normal bowel sounds. No rebound
or guarding.
Extremities show no edema. The AV fistula in the left forearm is nontender and palpation is normal.
Labs show white cell count of 20K with 85% polys, 2% bands. BUN/Cr is 77/6.5. Other electrolytes, including potassium, are normal. A chest x-ray is performed, which is normal. Blood is sent to the lab for culture.
You are puzzled until a small light suddenly flicks on in midair above your head representing a bright idea you are having.
Remembering something you learned as a hospital volunteer in junior high school, you scamper off to the laboratory, obtain a sample of the patient's blood, perform a quick Gram's stain while no one's paying attention, and slip the slide under a microscope.
At 100X magnification, you discover:
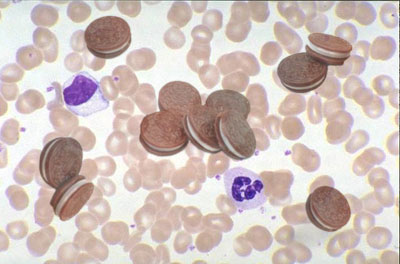
What's going on?
Answer:
Staph Oreos
This patient, an obese 65-year-old male on dialysis, has a Staph Oreos bacteremia.
Upon further questioning, the patient admits to eating about thirty Oreos in one sitting on the day prior to the onset of fevers.
Examination of the Gram's stain reveals the presence of more than 100,000 colony forming units of Staph Oreos, the tastebud-tempting chocolate wafers with delicious vanilla creme filling that millions have come to know and love.
You start the patient empirically on vancomycin intravenously, knowing that most Staph Oreos are not only resistant to methicillin, but also impossible to resist!
The final cuture result three days later will prove your intuition correct. Had you waited until then to start antibiotics, however, the situation may well have become a full-blown Staph Oreos Double Delight Peanut Butter & Chocolate sepsis.
Even worse, patients with dialysis fistulas are prone to develop the dreaded complication Creme-emia when Staph Oreos get lodged in their shunts.
Luckily, your patient goes on to full recovery, and is discharged home in hale and hearty health. Cautioning him to choose his snack cookies more wisely in the future, you close the book on another job well done.
More Stuff!
Get the Q Fever! Book!
The Q Fever! Store!: T-shirts, caps, mugs, and thongs!
Support The Q!
Subscribe to the Q Fever! Mailing List!
Contact Q Fever!
Remember: Quality Without The Q Is Just Uality!
Menu

